Dr Rajneesh Kapoor; M.D, D.N.B, Punjab Rattan Awardee, (born November 30, 1970) is a renowned cardiologist from India. He specializes in Interventional cardiology and is practicing as Chairman – Interventional Cardiology at Medanta The Medicity, Gurugram, India.
Early Life & Education
Born in the town of Patiala in Punjab, Dr Rajneesh Kapoor studied medicine at Government Medical College, Amritsar, Punjab, Guru Nanak Dev University. Subsequent to that he obtained his doctor in medicine degree from Government Medical College & Hospital, Patiala, Punjab, Punjabi University. He then got awarded as Diplomate of National Board from Escort heart Institute & Research Centre, New Delhi. He has accolades of merit scholarship by state education board in middle & high class.
Career
Dr Rajneesh Kapoor Joined Medanta The Medicity in the year 2010 and is at present practicing as Senior Director – Interventional cardiology. He is recognised for his contributions as a key player in setting up of centre operations & processes of cardiac catherization services at Medanta.
Prior to that he served as consultant in the department of cardiology at Escort heart Institute & research centre. He was responsible for planning, setting up & expanding the angiography & interventions program of the institute.
Awards & Recognitions
A complete blockage in a coronary artery is called a total coronary occlusion, or if it more than three months old, a chronic total occlusion.
Coronary Artery Disease is the narrowing or blockage of the coronary arteries caused by atherosclerosis.
Atherosclerosis is the buildup of cholesterol, fatty and inflammatory deposits (called plaque) on the inner walls of the arteries that restrict blood flow to the heart. Without adequate blood flow, the heart becomes starved of oxygen and vital nutrients it needs to work properly.
Angina is chest pain or discomfort that occurs when the heart isn’t receiving enough blood. It is a symptom of an underlying heart problem, usually coronary artery disease.
An aortic aneurysm is a bulging section in the aorta, the main artery that carries blood from the heart into the chest and abdomen. An aneurysm that grows too large may burst and cause bleeding.
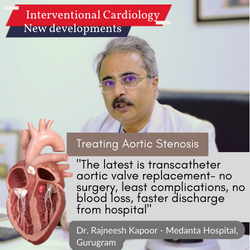
Aortic stenosis is a narrowing of the aortic valve that decreases blood flow into the aorta, the main artery carrying blood out of the heart.
No Incision, No Blood loss, no sedation, discharge from hospital in 3 days. Thoroughly explained by Award-winning #1 tavr/tavi specialist Dr. Rajneesh Kapoor - Vice-Chairman, Interventional cardiology at Medanta Hospital, Gurugram, India.
Most heart attacks start slowly and build up gradually over few minutes time. Heart attacks can be perceived as mild pain or discomfort, including pressure, squeezing, tightness, fullness or pain. The chest discomfort may radiate to the neck, jaw, or arm, and is usually associated with shortness of breath, nausea, diaphoresis and pallor. Diabetics and women may not have the typical symptoms of chest discomfort, and may have only few of the associated features (shortness of breath or nausea, etc)
Yes. A yearly exam should include a blood pressure check, lipid and cholesterol test and a discussion with your doctor about other risk factors. Your physician is likely to compute risk score to calculate your risk for coronary heart disease and inquire about family history of coronary heart disease. From there, you and your doctor can decide how often to follow up and what else you can do to improve your overall health.
What is a TAVR? (Also called TAVI)
This minimally invasive surgical procedure repairs the valve without removing the old, damaged valve. Instead, it wedges a replacement valve into the aortic valve's place. The surgery may be called a transcatheter aortic valve replacement (TAVR) or transcatheter aortic valve implantation (TAVI).
Valve-within-valve — How does it work?
Somewhat similar to a stent placed in an artery, the TAVR approach delivers a fully collapsible replacement valve to the valve site through a catheter.
Once the new valve is expanded, it pushes the old valve leaflets out of the way and the tissue in the replacement valve takes over the job of regulating blood flow.
How is TAVR or TAVI different from the standard valve replacement?
This procedure is fairly new and is FDA approved for people with symptomatic aortic stenosis who are considered an intermediate or high risk patient for standard valve replacement surgery. The differences in the two procedures are significant.his procedure is fairly new and is FDA approved for people with symptomatic aortic stenosis who are considered an intermediate or high risk patient for standard valve replacement surgery. The differences in the two procedures are significant.
What is involved in a TAVR procedure?
Usually valve replacement requires an open heart procedure with a “sternotomy.”, in which the chest is surgically separated (open) for the procedure. The TAVR or TAVI procedures can be done through very small openings that leave all the chest bones in place.
A TAVR procedure is not without risks, but it provides beneficial treatment options to people who may not have been candidates for them a few years ago while also providing the added bonus of a faster recovery in most cases. A patient's experience with a TAVR procedure may be comparable to a balloon treatment or even an angiogram in terms of down time and recovery, and will likely require a shorter hospital stay (average 3-5 days).
The TAVR procedure is performed using one of two different approaches, allowing the cardiologist or surgeon to choose which one provides the best and safest way to access the valve:
Entering through the femoral artery (large artery in the groin), called the transfemoral approach, which does not require a surgical incision in the chest, or
Using a minimally invasive surgical approach with a small incision in the chest and entering through a large artery in the chest or through the tip of the left ventricle (the apex), which is known as the transapical approach.
Eating right is a powerful way to reduce or even eliminate some heart disease risk factors. A heart-healthy diet can help cut total and LDL ("bad") cholesterol, lower blood pressure, lower blood sugar, and help you shed pounds.
Tips:
Smoking is a major risk for several diseases including heart disease, stroke, and several cancers. Even low-tar cigarettes and light smoking can increase the risk of heart disease substantially. There are now several alternative approaches to helping people stop smoking. These include nicotine-replacement patches and gum as well as oral medication.
If you are able to stop smoking, your risk of a heart attack or stroke decreases within a few weeks. The risk goes down to that of a nonsmoker within about two years. In addition, a lot of patients comment that they feel healthier and have more energy after they’ve stopped smoking.
Being overweight can increase the risk of heart disease in several ways. There can be a ten-fold increase in risks of high blood pressure and diabetes. In addition, being overweight will decrease the HDL or “good” cholesterol, which is now recognized as a major risk factor. If you are overweight, it is important to diet and exercise in order to lose weight and reduce these risk factors.
Consider a diet that is balanced among all the main food groups, with fat content making up no more than 30 percent of calories and most of that fat being unsaturated. Avoid a diet that restricts carbohydrates or fruits and vegetables, because this may adversely affect vitamin intake and blood cholesterol.
Red meat contains a lot of saturated fat. If you eat red meat every day, it is likely that your cholesterol is about 10-20 percent higher than it should be. Alternatives to red meat include chicken, fish, and turkey, as well as nonmeat protein sources like nuts and beans.
It usually takes two to four weeks for a change in diet to start to influence cholesterol levels. However, the full effect of a change in diet may not be seen for up to three months.




{kind=link}
{kind=link}